
Diffusion of Innovation Theory: What It Means for Your Health for life
Mar 30, 2026
I would like to consider myself an innovative person.
Before you picture someone who queues overnight for the latest tech release, let me clarify what I actually mean by that. My brain is wired for problem solving. I naturally make connections between seemingly unrelated ideas, and I think in systems, always tracing how one variable influences another, and how small shifts in behaviour can ripple outward in ways we don't always anticipate.
When something new lands in front of me, whether that's a change in how I manage my clinic, a new approach to breathwork, or a piece of technology promising to streamline my workflow, I don't panic. I don't dismiss it either. I take a moment to place it within my existing frame of reference and ask:
- Where does this fit?
- What problem does it solve?
- Does it move me closer to where I want to go?
And crucially, I don't need it to be perfect before I say yes.
This is something I've noticed particularly in how I run my businesses. I'll quite happily patch together three imperfect tools to approximate the one perfect tool that doesn't yet exist, while simultaneously advocating for better solutions and campaigning for the kind of innovation that would make that patchwork unnecessary. That willingness to accept good enough for now in service of forward momentum is, I've come to understand, a hallmark of a particular kind of thinker.
But here's the thing: that isn't everyone. And honestly, it shouldn't be.
Human beings are wonderfully varied in how they respond to change. What feels energising and natural to one person feels overwhelming and threatening to another. Neither response is wrong. Understanding the difference, however, is one of the most practically useful things I've ever learned, both as a clinician and as a person trying to build sustainable change in my own life.
What Is the Diffusion of Innovation Theory?
In 1962, communication scholar Everett Rogers published one of the most cited academic works of the 20th century: Diffusion of Innovations. His central question was deceptively simple:
Why do some ideas spread, and others don't?
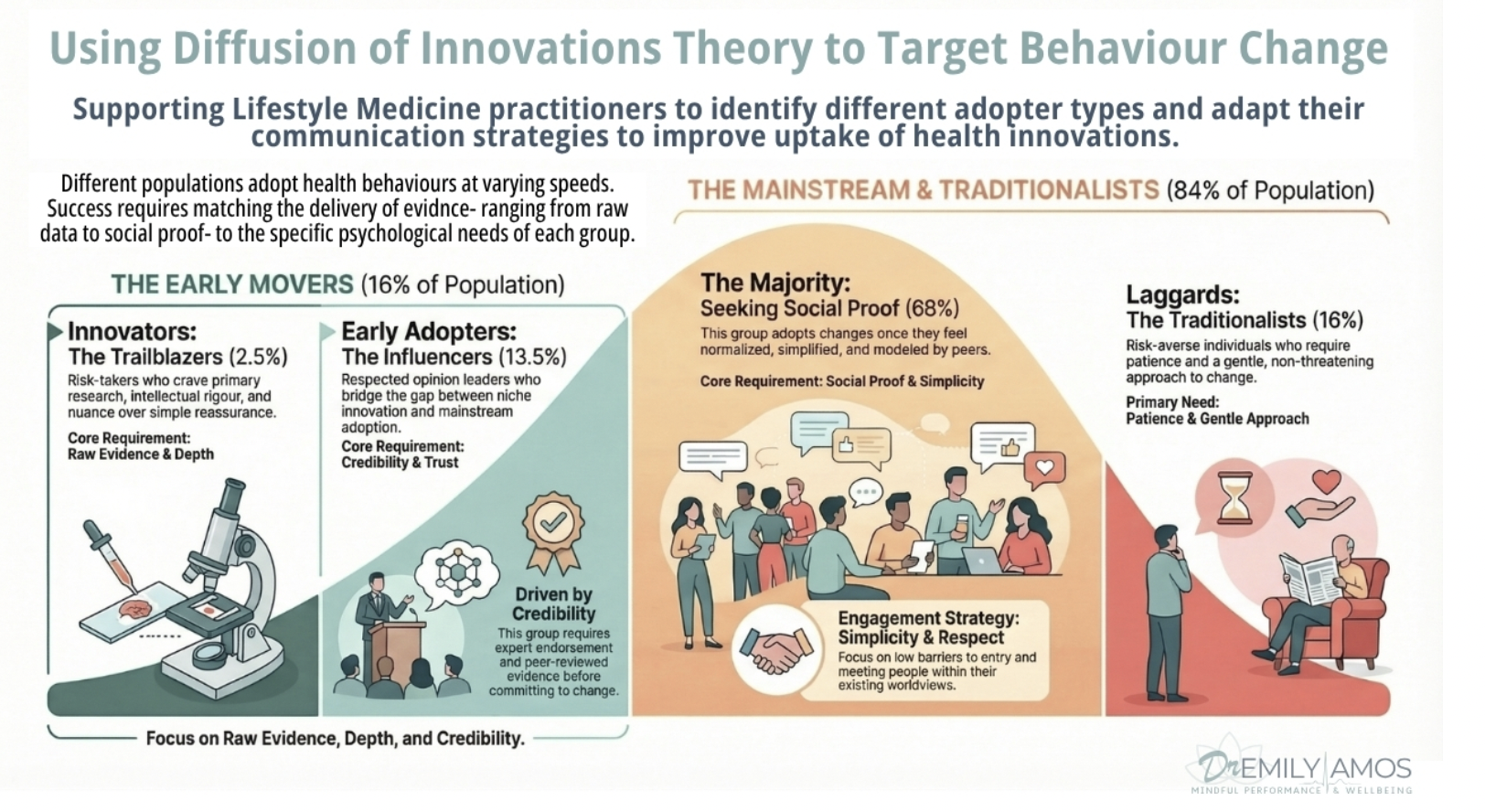
Rogers found that when any new idea, behaviour, or technology enters a population, adoption doesn't happen all at once. Instead, it ripples outward in a predictable, observable pattern across five distinct groups of people. Each group has its own relationship with change, its own motivations, and its own set of needs that must be met before adoption becomes possible.
Understanding those groups changed the way I practise. Because in lifestyle medicine, mindfulness, and stress management, I am, every single day, in the business of asking people to change. And change, as it turns out, is far more nuanced than simply presenting someone with a compelling idea and expecting them to act on it.
The research bears this out. Behaviour change science tells us that knowledge alone is rarely sufficient to shift behaviour. People need relevance, readiness, social context, and a sense of safety before they will genuinely commit to something new. The Diffusion of Innovation Theory gives us a practical map for understanding where someone sits within that process, and how to engage with them accordingly.
The Five Adopter Groups
1. Innovators (approximately 2.5% of the population)
Innovators are the trailblazers and experimenters. They will engage with a new mindfulness-based programme the week it launches, commit to a structured sleep optimisation protocol based on early but promising research, or explore an emerging behavioural intervention long before it has entered mainstream clinical practice.
Key characteristics of innovators:
- High tolerance for risk and ambiguity
- Comfortable with uncertainty and even with failure
- Well-networked with others who share their appetite for the new
- Motivated by curiosity and possibility rather than social proof
In a clinical context, innovators are often the patients who arrive having already read the primary research on their condition and ask about interventions I haven't yet raised. They are energising to work with, genuinely so, but they also require a particular kind of engagement. Enthusiasm must be matched with rigour. The goal is to honour their curiosity while ensuring we are building on evidence-informed foundations rather than simply chasing novelty for its own sake.
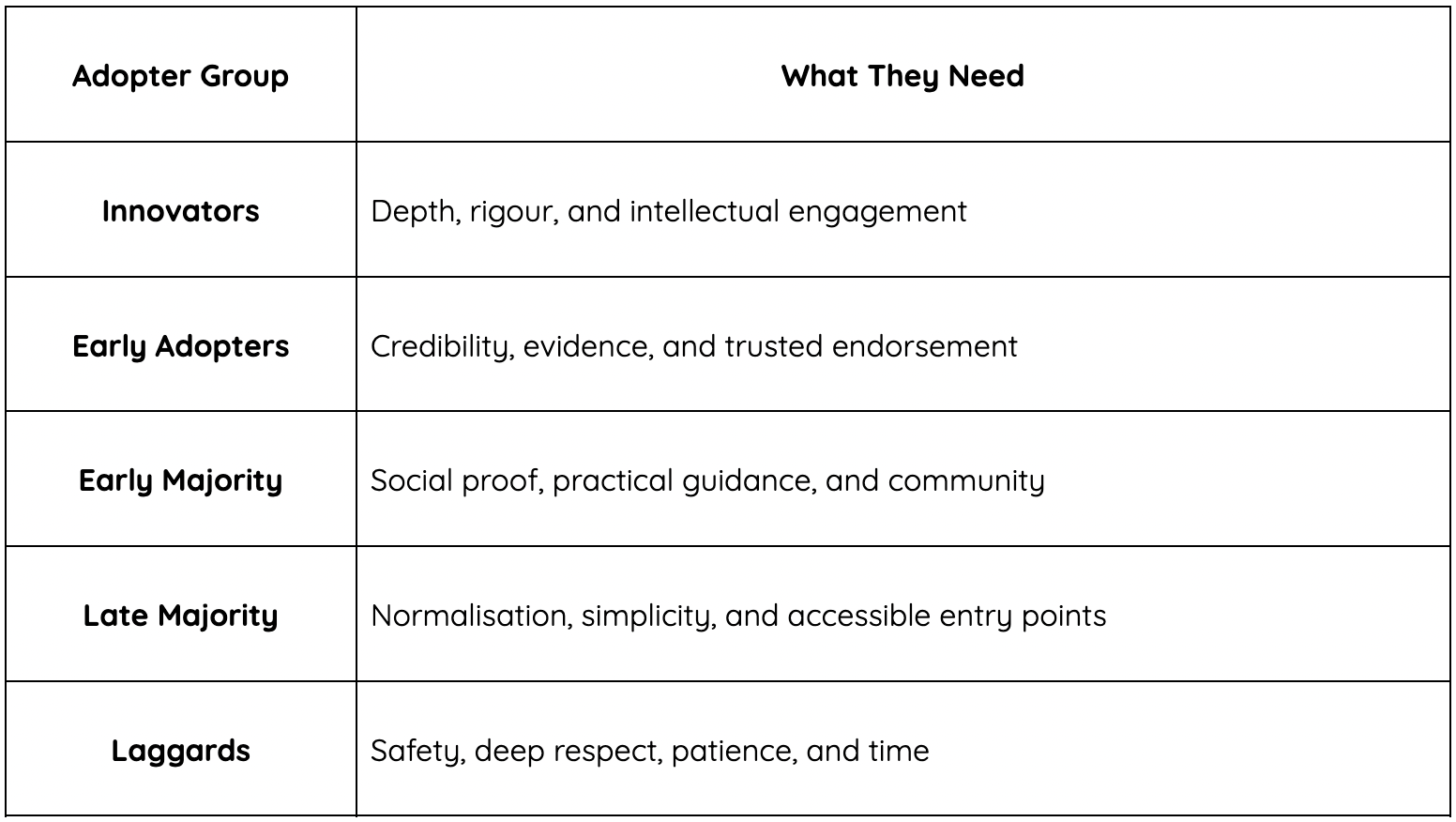
What innovators need: Depth, intellectual rigour, and a practitioner or guide who can keep pace. They want access to primary evidence, not just summaries. They want nuance, not reassurance.
2. Early Adopters (approximately 13.5% of the population)
Early adopters are arguably the most influential group in the entire model, and the one that wellness professionals should understand most deeply.
They are not quite as experimental as innovators. They prefer to see a degree of evidence before committing. But once they are convinced, they move with conviction, and they bring others with them. Critically, early adopters tend to be respected opinion leaders within their communities. They are the people their friends, colleagues, and family members turn to and ask: "But what do you actually think? Is this worth trying?"
In wellness terms, early adopters were engaging with Mindfulness-Based Stress Reduction (MBSR) and evidence-based exercise prescriptions for mental health long before these practices were embedded in clinical guidelines or discussed in mainstream media. They read widely, reflect carefully, and when they integrate a well-evidenced practice into their lives, the people around them notice and often follow.
The influence of early adopters is difficult to overstate. They are the bridge between the innovative fringe and the broad population. Without them, ideas and practices, however well-evidenced, often stall.
What early adopters need: Credibility above all else. Peer-reviewed evidence, expert endorsement, and clear alignment with their values. They don't require something to be mainstream. They require that the source be trustworthy and the evidence sound.
3. Early Majority (approximately 34% of the population)
This is the group where mass adoption either takes root or stalls entirely. The early majority represent a substantial portion of the population, and reaching them effectively is what determines whether a health behaviour becomes genuinely widespread.
Early majority adopters are thoughtful, practical, and community-oriented. They look to early adopters for their cues, and they want to see something working for real people, people like them, before they invest their time, energy, or trust in it.
This group began practising mindfulness meditation when a trusted colleague shared their experience of a structured programme, or when their GP mentioned that evidence-based stress reduction techniques had measurable, documented impacts on blood pressure and cardiovascular risk. They are not resistant to change. They are simply deliberate and relational in how they approach it. Social proof, in other words, carries more weight than abstract research findings.
In my practice, the majority of the people I work with sit somewhere in this space. They understand, intellectually, that lifestyle change will serve them. They have often read articles, listened to podcasts, or had conversations that have planted the seed. What they need is to see it modelled, explained, and made genuinely accessible before they will fully commit.
What the early majority needs: Social proof, practical guidance, and evidence that is delivered with warmth and relevance rather than clinical detachment. Community is a powerful motivator here. Consistency matters more than intensity, and pressure, however well-intentioned, tends to backfire.
4. Late Majority (approximately 34% of the population)
The late majority adopt new practices largely because the social pressure to do so eventually outweighs the discomfort of changing. They are sceptical by nature, not stubborn, but cautious. Many have experienced health trends, wellness fads, or organisational changes that promised transformation and delivered very little. That history of disappointment produces a healthy, if sometimes inconvenient, resistance to the new.
By the time the late majority begin exploring mindfulness or structured relaxation practices, these approaches are on the school curriculum, available through their GP surgery, covered by their health insurer, and recommended by multiple trusted people in their social and professional circles.
The tipping point here is not enthusiasm. It is normalisation. When something stops feeling like a trend and starts feeling like a standard, the late majority will begin to engage.
What this group needs from practitioners and wellness professionals is not evangelism, advocacy, or urgency. Those approaches tend to entrench resistance rather than dissolve it. What works is simplicity, reassurance, and the lowest possible barrier to entry.
One minute of diaphragmatic breathing before sleep. A single, guided body scan. A brief walking practice that requires no equipment, no class booking, and no previous experience. Something so achievable that the perceived risk of failure feels negligible.
What the late majority needs: Simplicity and normalisation. Short, accessible entry points into well-evidenced practices. Reassurance that this is not a dramatic overhaul but a small, manageable addition. Trust is earned slowly here and must never be assumed.
5. Laggards (approximately 16% of the population)
Let's be careful with this label. "Laggard" sounds pejorative, and the connotation is unfair. These are not people who are ignorant, stubborn, or beyond reach. They are people with a particular relationship with change, one that prioritises the known over the new, the proven over the promising.
Laggards are the last to adopt any innovation, and they often do so only when the previous way of doing things is simply no longer available to them. They tend to be deeply traditional in their values, highly risk-averse, and anchored in what has consistently worked rather than in what might work.
In health terms, this might look like the patient who firmly resists any conversation about psychological stress as a contributor to physical illness, despite a substantial and well-replicated body of research linking chronic stress to cardiovascular disease, immune dysregulation, and metabolic dysfunction. It might look like the person who will only engage with their health through a purely biomedical lens, and for whom any mention of mindfulness, lifestyle medicine, or behavioural intervention feels at best unnecessary and at worst faintly suspicious.
They are not wrong for thinking this way. Their framework has served them, and change feels genuinely threatening. Treating that response with impatience or dismissiveness is both clinically unhelpful and ethically unkind.
What laggards need: Patience, respect, and a willingness to meet them entirely within their existing worldview before you attempt to expand it. Any widening of the aperture must be gentle, gradual, and led by the patient, not the practitioner. Sometimes the most powerful clinical act is to plant a seed thoughtfully and leave the door open, without expectation.
Why This Framework Matters
The Diffusion of Innovation Theory dismantles one of the most persistent and damaging myths in health promotion:
If you just give people good enough information, they will change.
They won't. Not all of them. Not all at once, and not through the same pathway.
Mindfulness-based interventions offer a clear and well-documented illustration of this. The evidence base is robust, spanning thousands of peer-reviewed studies and demonstrating consistent benefits across stress reduction, anxiety, depression, chronic pain, and cardiovascular health, and yet, adoption has never been purely evidence-led. It has always been social, contextual, and deeply human in how it has spread.
Mindfulness reached the mainstream because innovators engaged with early MBSR research and clinical trials in the 1980s and 1990s. Early adopters gave the practice credibility within their professional and social networks. The early majority normalised it through lived, visible experience in workplaces, schools, and healthcare settings, and the late majority eventually encountered it in the institutional contexts they already trusted: their GP's surgery, their employer's wellbeing programme, their child's school.
That process took decades. It required different messengers, different framings, and different entry points at every stage of the journey.
What This Means for You
Whether you are a clinician, a wellness professional, a manager trying to embed a culture of genuine wellbeing in your team, or simply someone trying to help a resistant loved one take their stress load seriously, this framework has direct and practical relevance.
Before your next conversation about behaviour change, pause and ask: which group is this person most likely in? What do they actually need from me right now?
None of these needs is wrong. They are simply different, and the practitioners, leaders, and communicators who understand that difference are consistently more effective than those who deliver the same message, in the same way, to everyone.
The most powerful thing any of us can do in the service of lasting health change is to meet people where they actually are, rather than where we wish they were.
That is not a compromise of our expertise or our standards. It is the fullest expression of them.
Stay connected with news and updates!
Join the mailing list to receive the latest blogs, news and updates.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
